

Damage of the facet joint, which connects the bones we call the vertebrae that forms the spine, due to degenerative and traumatic causes, localized in the neck or waist, or rarely spread to the anterior and posterior aspects of the legs, It is one of the most important causes of neck pain. When the cause of pain is determined to be facet joints, long-term or permanent treatment can be provided with facet joint blockade and then radiofrequency thermocoagulation (RFT).
Procedure
The procedure should be performed in the operating room under imaging (C-arm fluoroscopy). You must be hungry 4 hours before the procedure. Your vital functions will be followed by an anesthesiologist in the operating room. After the pain reliever and sedation medication is administered intravenously, the procedure is started.
For facet joint blockage, after visualizing the joints with C-arm fluoroscopy, the facet joint is accessed with a 10 cm long needle following local anesthesia. The procedure is completed by applying local anesthetic cortisone.

-Facet Intra-Articular Injection-
At least 50% or more relief is expected in the patient’s pain after the block. Once the local anesthetic effect wears off, the patient’s pain may begin again. If cortisone was used, the pain starts to decrease again after 24-48 hours.
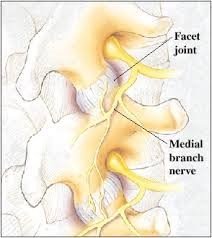
If the patient’s pain has decreased at the desired level after local anesthetic application, long-term relief can be achieved with RFT application. This application can be done in the same session immediately after the facet block, or it can be applied 1-2 weeks later. The procedure is performed in the operating room like facet block injection. Again, the entry site is determined under imaging, and the median facet nerves are reached with special RF needles, and the pain-bearing fibers of the nerve are numbed with heat with the RFT device.

-Facet Medial Branch RFT-
Things to Consider Before the Procedure:
For sedation applications, it is necessary to fast for 4 hours before the procedure .
Blood pressure medications should be taken on the morning of the procedure with very little water. Blood thinners such as Aspirin® and Coraspin® should be discontinued 1 week in advance.
What to do after the procedure:
It is sufficient to rest for 1-2 hours after the procedure.
The complaint of reduced pain after the intervention may start again within 4-6 hours. This is due to the fact that the effect of the local anesthetic has disappeared.
The main effect of long-acting cortisone reaches the desired level within 48-72 hours and the pain begins to decrease within 3-4 days.
On the other hand, in RFT applications, pain complaints begin to decrease significantly within 3-4 days and relief is achieved within 1 week-10 days.
It is necessary to avoid movements that will put excessive strain on the waist or neck for 2-3 days after the intervention.
Painkillers can be used for 2-3 days if there is a complaint of pain
What are the Risks of the Procedure?
Although the most important risk is infection, it is a very rare side effect that can be seen only once in 70-80 thousand patients. In such cases, antibiotic treatment should be started. Temporary loss of sensation in the hip and upper leg may be seen in patients undergoing RFT. Depending on the cortisone used, fluid retention in the body and deterioration in the sugar pattern can be observed for 1-2 weeks in patients with diabetes.
To Whom Does It Not Apply?
Those who have systemic infection at the intervention site
Those who do not want the intervention